BPC-157 vs TB-500
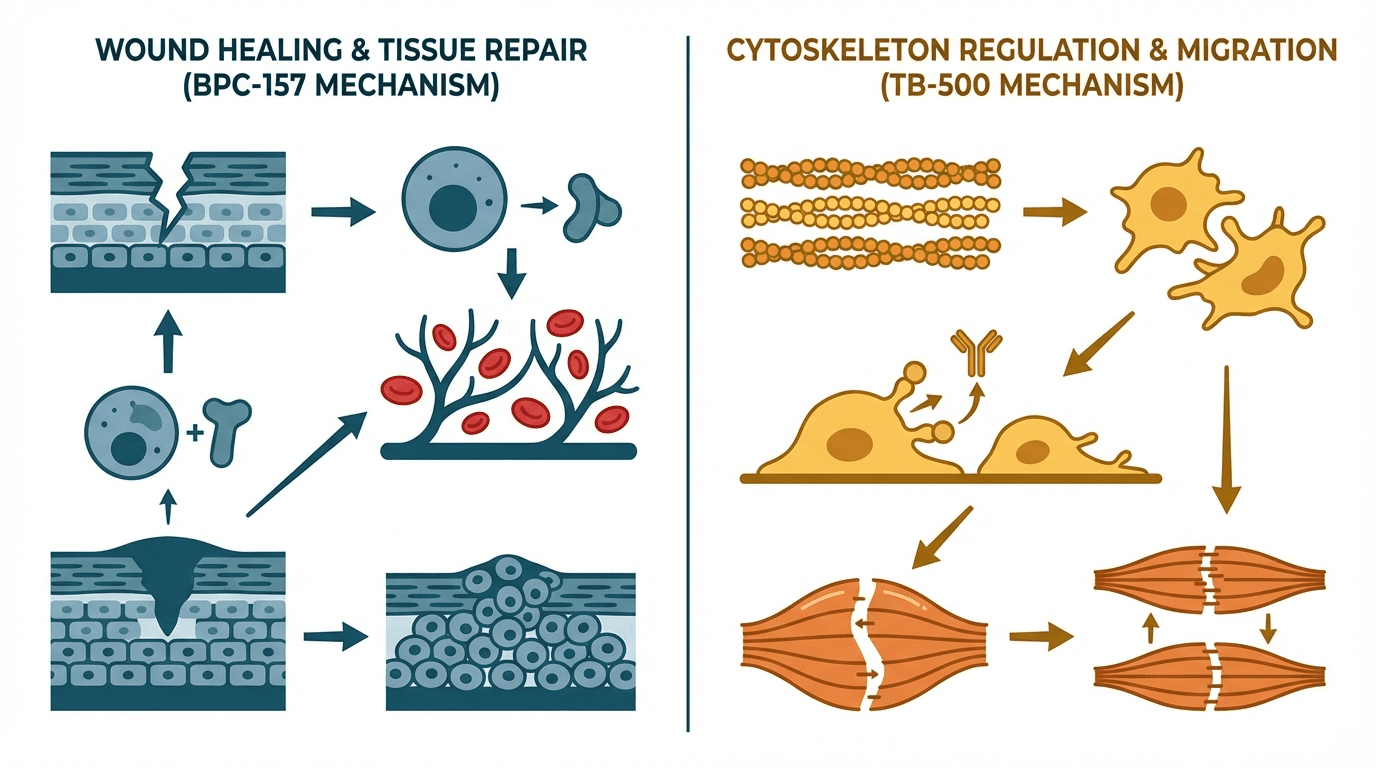
BPC-157 and TB-500 are the two most popular peptides for healing and tissue repair. BPC-157 excels at localized healing — especially tendons, ligaments, and gut tissue — through angiogenesis and growth hormone receptor upregulation. TB-500 provides systemic healing via actin upregulation and cell migration, making it better for widespread or hard-to-reach injuries. Many users stack both for synergistic results.
Head-to-Head Comparison
| Criteria | BPC-157 | TB-500 |
|---|---|---|
| Primary mechanism | Angiogenesis + GH receptor upregulation | Actin upregulation + cell migration |
| Best for | Localized injuries (tendons, gut, specific muscle tears) | Systemic/widespread injuries, cardiac repair, flexibility |
| Route of administration | Subcutaneous, oral, or intramuscular | Subcutaneous or intramuscular only |
| Typical dosage | 200–500 mcg, 1–2× daily | 2.0–2.5 mg, 2× weekly |
| Half-life | ~4 hours | ~6–8 hours |
| Injection location matters? | Yes — inject near injury site for best results | No — systemically active regardless of injection site |
| Oral bioavailability | Yes (stable in gastric acid) | No (must be injected) |
| Gut healing | Excellent — primary use case | Limited evidence for gut-specific healing |
| Hair growth potential | Minimal evidence | Preliminary evidence (stem cell activation in follicles) |
| Research status | Preclinical (extensive animal data) | Preclinical (extensive animal data) |
| WADA banned? | Not currently listed | Yes — banned in and out of competition |
| Approximate monthly cost | $40–$80 | $60–$120 |
When to Choose Each
Verdict
For targeted healing of a specific injury (torn tendon, gut issues, localized muscle damage), BPC-157 is the stronger first choice due to its localized action and oral bioavailability. For systemic healing, widespread inflammation, cardiac support, or injuries in hard-to-reach areas, TB-500 is preferred. The optimal approach for serious injuries is stacking both peptides — BPC-157 for local repair and TB-500 for systemic support — which is the most common protocol among experienced users.
References
Frequently Asked Questions
Can I stack BPC-157 and TB-500 together?
Which is better for tendon injuries?
Which is better for gut issues?
Do I need a prescription for BPC-157 or TB-500?
How long does a typical BPC-157 or TB-500 cycle last?
Explore next
- BPC-157 dosage guideComprehensive BPC-157 dosage guide covering subcutaneous, intramuscular, and oral administration protocols. Includes reconstitution instructions, cycle guidance, stacking considerations, and references to published preclinical research on this gastric pentadecapeptide.
- TB-500 dosage guideEducational reference covering TB-500 (Thymosin Beta-4) dosage protocols, including loading and maintenance phases, reconstitution, and administration details as discussed in research literature.
- Reconstitution CalculatorCalculate exactly how many units to draw on your syringe. Enter your vial size, bacteriostatic water volume, and desired dose.
- Dosage CalculatorFind evidence-based dosing ranges for any peptide. Adjust for body weight, experience level, and administration route.
- Cost CalculatorEstimate peptide costs per dose, per week, per month, and per year. Enter your vial price and dosing schedule to plan your budget.