Ipamorelin vs Sermorelin
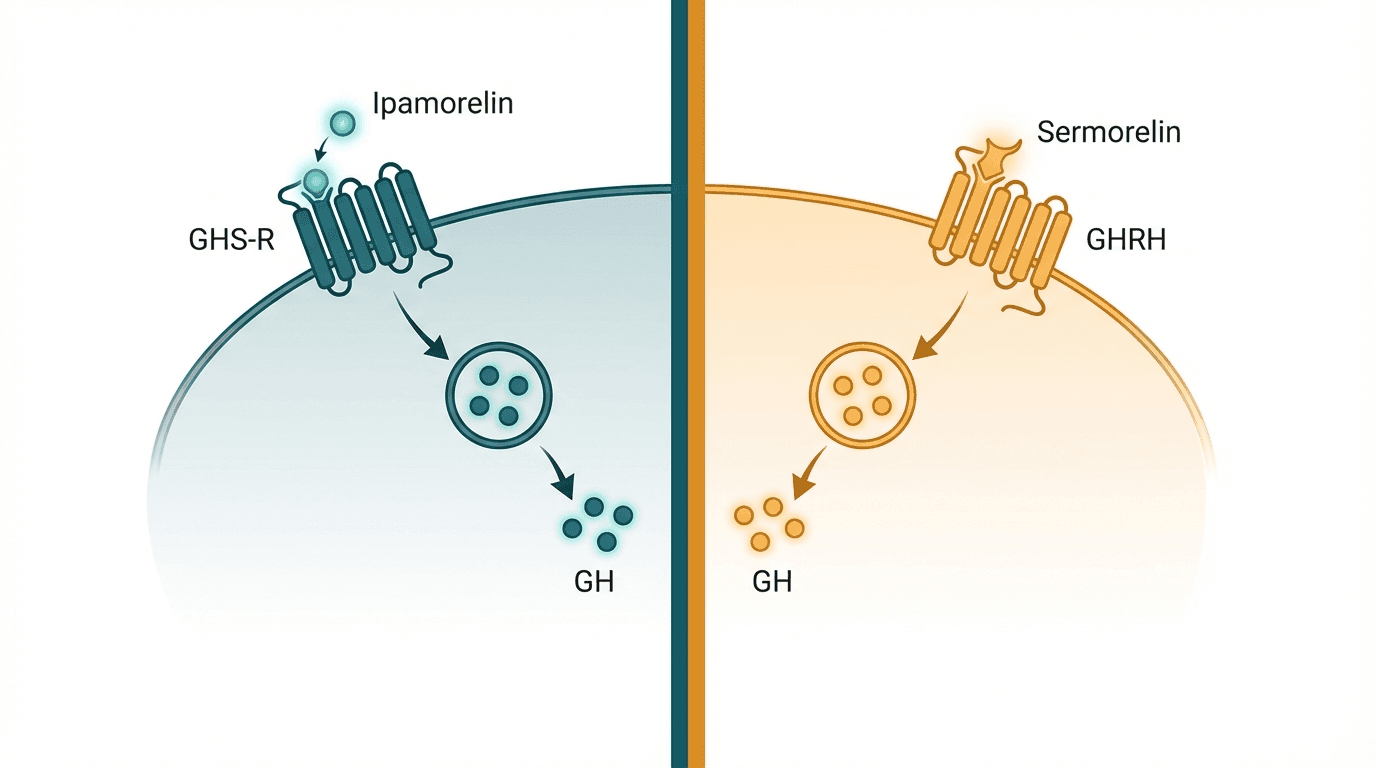
Ipamorelin and sermorelin both stimulate natural growth hormone release but work through entirely different receptor pathways. Ipamorelin is a selective growth hormone releasing peptide (GHRP) that mimics ghrelin at the pituitary level without significantly raising cortisol or prolactin, while sermorelin is a growth hormone releasing hormone (GHRH) analog that acts on the GHRH receptor to trigger GH secretion. Because they target different receptors, the two are often stacked for a synergistic GH pulse far greater than either peptide alone.
Head-to-Head Comparison
| Criteria | Ipamorelin | Sermorelin |
|---|---|---|
| Primary mechanism | Selective ghrelin receptor (GHS-R1a) agonist at the pituitary | GHRH receptor agonist — mimics endogenous GHRH(1-29) |
| Peptide class | Growth hormone releasing peptide (GHRP) | Growth hormone releasing hormone (GHRH) analog |
| Selectivity | Highly selective — minimal cortisol and prolactin elevation | Moderate selectivity — slight cortisol and prolactin increase possible |
| Typical dosage | 200–300 mcg subcutaneous, 1–3× daily | 200–300 mcg subcutaneous, once daily before bed |
| Half-life | ~2 hours | ~10–20 minutes |
| GH release pattern | Strong, clean GH pulse with fast onset | Physiologic GH pulse that mimics natural GHRH signaling |
| Effect on hunger | Minimal appetite increase despite ghrelin mimicry | No significant appetite stimulation |
| FDA history | No FDA approval; research chemical / compounding use | Previously FDA-approved (Geref) for pediatric GH deficiency; brand discontinued but available via compounding |
| Side effect profile | Very mild — occasional headache, transient flushing at injection site | Mild — injection site reactions, facial flushing, headache, dizziness |
| Synergy with other peptides | Commonly stacked with CJC-1295 or sermorelin (GHRH + GHRP synergy) | Commonly stacked with ipamorelin or GHRP-2 for amplified GH pulse |
| Research depth | Moderate — multiple clinical studies on GH release and safety | Extensive — decades of clinical data, former FDA-approved drug |
| Approximate monthly cost | $40–$80 (research grade); $150–$350 (clinic) | $50–$100 (research grade); $200–$400 (clinic) |
When to Choose Each
Choose Ipamorelin
Users who want clean GH elevation with minimal side effects, those sensitive to cortisol or prolactin increases, bodybuilders seeking lean mass gains without appetite disruption
Choose Sermorelin
Anti-aging clinic patients wanting a well-studied GH secretagogue, physician-supervised protocols, those who prefer a peptide with FDA-approval history
Verdict
Ipamorelin is the better choice for most users seeking clean, targeted GH elevation with minimal side effects — its selectivity means virtually no unwanted cortisol or prolactin spikes. Sermorelin is the better-studied option with a longer clinical track record and FDA history, making it preferred by physicians who want established safety data. The optimal approach for maximizing GH release is stacking ipamorelin with sermorelin (or CJC-1295), combining GHRP and GHRH pathways for a synergistic effect that can amplify GH output 3–5× beyond either peptide alone.
References
- Ipamorelin, the first selective growth hormone secretagogue (1998) — PubMed
- Growth hormone releasing peptides: clinical and basic aspects (1999) — PubMed
- Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency (1999) — PubMed
- Safety and efficacy of ipamorelin for cardiovascular surgery patients (2008) — PubMed
- Growth hormone-releasing hormone and growth hormone secretagogues: therapeutic and diagnostic applications (2007) — PubMed
Frequently Asked Questions
Can I stack ipamorelin and sermorelin together?
Which peptide has fewer side effects?
How long before I see results from ipamorelin or sermorelin?
Why was sermorelin discontinued as an FDA-approved drug?
Which is more cost-effective, ipamorelin or sermorelin?
Explore next
- Ipamorelin dosage guideEducational reference for ipamorelin dosage protocols, optimal timing, and administration guidelines as discussed in published research studies.
- Sermorelin dosage guideComplete sermorelin dosage guide with injection protocols, bedtime timing rationale, 5-on/2-off cycling strategy, reconstitution instructions, and stacking considerations. Covers standard and higher dose protocols based on published research and clinical use patterns.